In a departure from my standard posts on this site, I am sharing a piece I wrote about the predictive value of Theta waves.
Delta and Theta brainwaves are foundational. During our early years, they are dominant, but as we age, they become more situational. After about age seven, we require Delta and Theta waves for sleep and introspection, but when they are dominant during our waking hours, it causes our thinking to be slow and our wits to be dull. TBIs can contribute to dominant slow waves, but research shows there is hope. Here’s what I’ve learned:
In a study done by Princhep, et al, healthy folks (bloodwork and psychiatric evaluations within norms) over 60 years old were given an assessment called the GDS – Global Deterioration Scale.
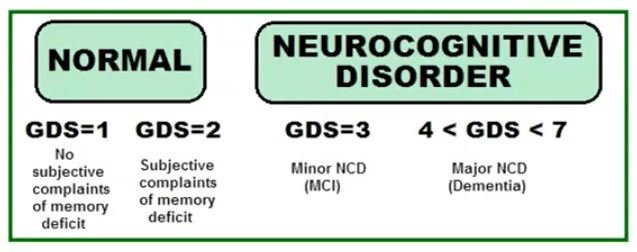
The GDS is a way for clinicians and researchers to evaluate cognitive decline. Those who score a 2 on the GDS may report concerns about memory loss – “I forgot where I parked the car” – but there are no external indicators of decline.
The researchers gave those who scored 2 or lower on the GDS – a total of 44 people – a quantitative electroencephalogram, also known as a qEEG or simply Q* – an assessment I administer here at Hive Mind.
Ten years later the same people were reassessed with both the GDS and the qEEG.
Seventeen of the group of 44 still scored 2 or lower on the GDS while 27 scored higher, meaning they were showing clinical signs of dementia. When the Qs were compared, a difference between the two groups became clear. The 27 people who were in obvious decline had all exhibited excess Theta ten years earlier. Of the 17 who remained cogent, none had had the excess Theta.
Then the researchers became proactive, working with another group of at-risk elders – people who met the previous criteria of good health and only mild memory complaints but who had high Theta in their Qs. They divided the group in two and gave one set of folks neurofeedback to “down train” or discourage too much Theta. The other set received “sham” feedback, meaning they didn’t get Theta down protocol. Each person received a total of 30 thirty-minute sessions.
The results were impressive. The group receiving actual Theta down training maintained their cognitive capabilities in follow-ups that occurred at two months and one year while the group receiving sham feedback did not fair as well cognitively. The researchers wanted to extend the follow-up for another year but the folks in the sham feedback group were not interested in continuing. Why would they?**
Aside from TBIs, there are a few factors that can contribute to increased Theta activity such as poor sleep and increased anxiety, so approaching excess Theta from several fronts is advisable, and neurofeedback is a warranted component.
*A qEEG collects a person’s eeg both while their eyes are closed and while they are open. Then the eeg is run through a normative database comparing the information to eegs from brains sharing the same age and gender.
**Several years ago, I attended a lecture by Dr. Bessel van der Kolk. He described a situation that arose during a research project that was being done in his Boston clinic. Clients were receiving either neurofeedback or sham neurofeedback and the clinicians were blinded to the details, meaning they did not know who was or wasn’t receiving training. Well into the research, a snowstorm hit Boston, dumping a tremendous about of snow and making travel in the city extremely difficult. Despite the impediment, people who were receiving neurofeedback showed up at the clinic, asking for their sessions while the people receiving sham “treatments” did not make the effort.
Prichep LS, John ER, Ferris SH, Rausch L, Fang Z, Cancro R, Torossian C, Reisberg B. Prediction of longitudinal cognitive decline in normal elderly with subjective complaints using electrophysiological imaging. Neurobiol Aging. 2006 Mar;27(3):471-81. doi: 10.1016/j.neurobiolaging.2005.07.021. Epub 2005 Oct 6. PMID: 16213630.

Leave a comment